Pancreatic Cancer
For Patients
Pancreatic cancer is relatively uncommon, accounting for only 2.7% of all cancer cases in Australia. Therefore, some people may not fully understand the role of the pancreas and how cancer can develop here. This section outlines the functions of the pancreas, as well as important information about pancreatic cancer, including possible causes, diagnosis and treatment.
Where does it spread?
When a cancer spreads beyond the organ it originated in it is known as metastatic cancer.
A major concern when diagnosing a pancreatic cancer is whether or not the cancer has already spread (metastasised) outside of the pancreas. The location of the metastases will also determine whether the cancer is able to be surgically removed (resectable) or unable to be surgically removed (unresectable).
There are certain sites that pancreatic cancer may spread to, but every person may be different. Some of the common sites are:
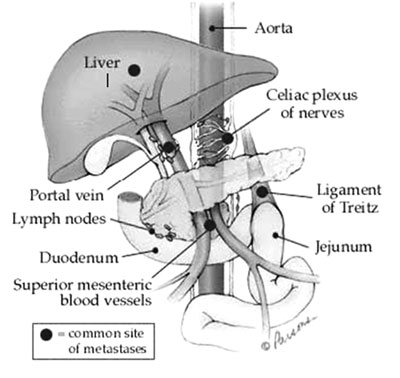
Lymph Nodes:
Metastases (mets) to lymph nodes does not automatically eliminate surgery as a treatment option. There are lymph nodes scattered throughout the body. The location of the affected lymph nodes makes a big difference for example the spread to more distant lymph nodes such as those near the liver, may mean the tumour is unresectable.
Liver:
Mets to the liver are a common finding especially with tumours in the tail and the body of the pancreas. Usually, if there is evidence of liver “mets”, surgery will not be an option.
Coeliac Plexus:
This is a network of many nerves that are grouped around the aorta where it passes through an opening in the diaphragm. These nerves can be pressed upon by a growing tumour, causing pain. This can be relieved by injecting alcohol into the nerves to stop the pain.
Portal Vein:
This is another important blood vessel that runs right next to the pancreas. It carries oxygen poor blood to the liver where the blood is filtered. If the cancer has spread to involve the portal vein, the cancer may be considered unresectable. The surgeon may decide that surgery can proceed. If so, they can remove the affected portion of the portal vein and replace it with an artificial graft.